What Is Macular Degeneration? A Complete Guide for Patients and Families
If you've just heard the words "macular degeneration" — from your eye doctor, from a family member's diagnosis, or from your own research after noticing changes in your vision — you're in the right place. This guide walks through everything in plain language: what macular degeneration actually is, the two types, what causes it, what symptoms to watch for, how it's diagnosed, and what can be done. Take your time. There's a lot here, but none of it is as overwhelming as the silence between you and the answers.
Reviewed by the eyehealth-today.com editorial team · Last updated: May 2026 · 12 minute read
What Is Macular Degeneration? Understanding the Macula
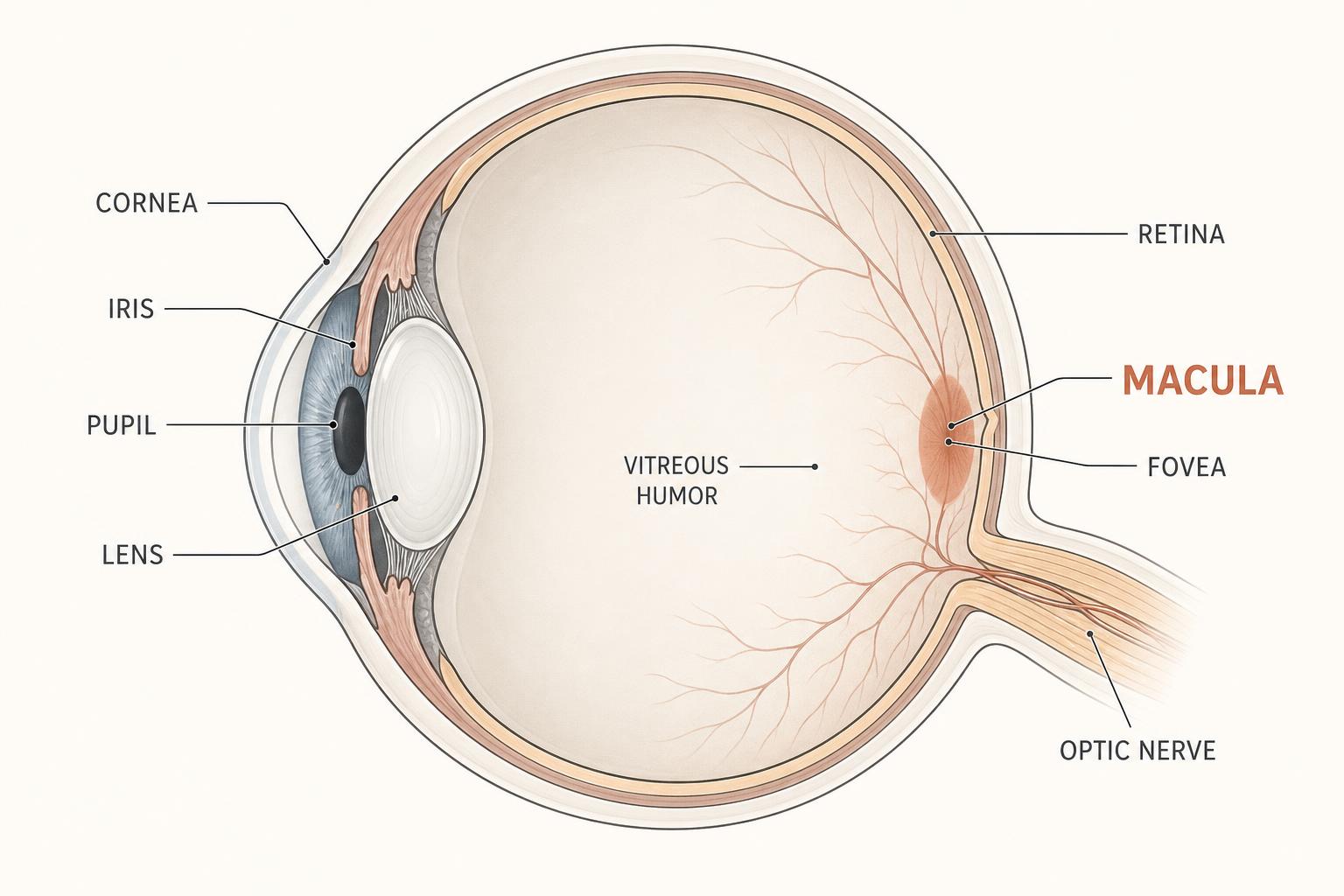
Macular degeneration is a progressive eye condition that affects the macula — the small central portion of the retina responsible for sharp, detailed central vision. It's the most common cause of vision loss in adults over 50, and it tends to develop slowly over years, sometimes decades.
The macula itself is roughly the size of a pencil eraser, but it does an outsized share of the work your eyes perform every day. It's responsible for the vision you use to read a book, recognize a face across a room, watch television, thread a needle, drive a car, or read your phone. When the macula is damaged, those tasks become difficult or impossible. Peripheral vision — the ability to see movement and shapes to the side — is handled by different parts of the retina and is usually unaffected.
This distinction matters more than almost anything else in this guide. Macular degeneration does not cause total blindness in most cases. Even in advanced stages, peripheral vision typically remains intact. People living with AMD navigate rooms, recognize loved ones at distance, and live independently for years and decades after diagnosis. The vision loss is real and significant, but it is not the catastrophic darkness many people imagine on the day they first hear the diagnosis.
It's worth distinguishing AMD from the two other common eye conditions older adults often confuse it with. Glaucoma damages the optic nerve, usually due to pressure inside the eye, and tends to affect peripheral vision first. Cataracts are a clouding of the lens — generally treatable with a routine surgical procedure. Macular degeneration is different from both. It affects the retina itself, and while there are now treatments that can slow some forms of it, the damage to existing retinal tissue is generally not reversible.
The "age-related" part of the name is statistical, not philosophical. About 85% of cases occur in adults over 60, and the risk climbs sharply with each decade after that. According to the National Eye Institute, roughly 19.8 million Americans over 40 have some form of AMD, and approximately 1 in 3 adults over 75 has it in some stage. The American Academy of Ophthalmology provides additional patient-facing material on the condition.
The Two Types: Dry vs Wet Macular Degeneration
Macular degeneration comes in two distinct forms — and the difference between them shapes nearly everything about how the condition is monitored and treated. Most people don't learn the distinction until they're diagnosed. Here it is, plainly.
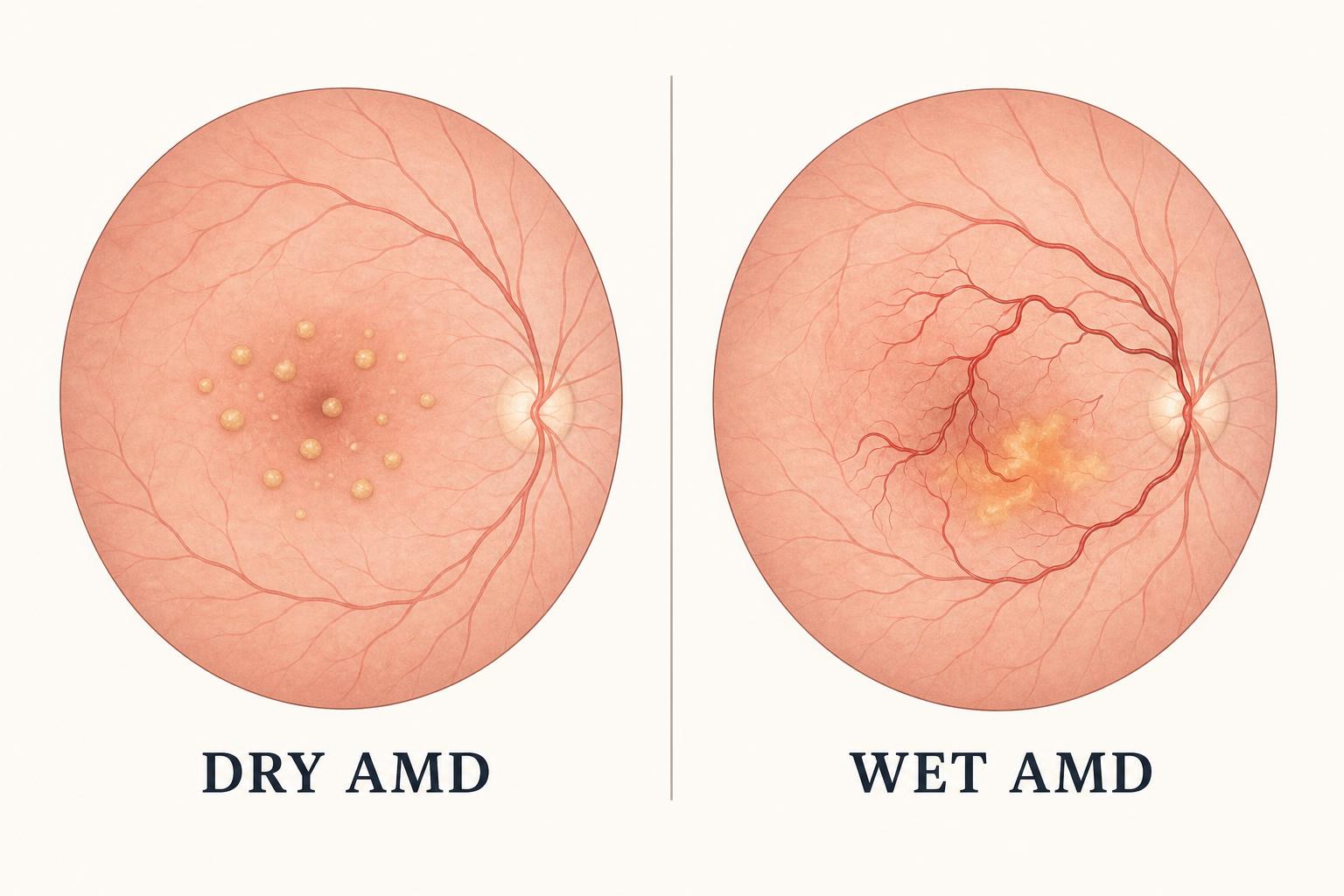
Dry AMD (atrophic, about 85–90% of cases)
The dry form is by far the more common type, and it progresses slowly — typically over years or decades. It's caused by the gradual thinning of the macula combined with the accumulation of small yellow deposits called drusen beneath the retina. Drusen are made of fats and proteins the eye fails to clear over time, and they interfere with the retina's ability to function normally.
Progression varies dramatically from person to person. Some people with dry AMD remain stable for decades with only mild symptoms. Others progress more quickly through the stages. Early symptoms are easy to dismiss as ordinary aging: needing brighter light to read, slight blurring of central vision, more difficulty adapting from a sunny street to a dim restaurant. This is part of why dry AMD is often first detected during a routine eye exam rather than a symptom-driven visit.
Wet AMD (neovascular or exudative, about 10–15% of cases)
The wet form is less common but more aggressive. It develops when abnormal blood vessels grow underneath the retina and begin to leak fluid or blood into the macular tissue. This leakage can cause rapid central vision loss — sometimes over days or weeks rather than years.
Standard medical treatment for wet AMD is anti-VEGF injections — medications such as Avastin, Lucentis, or Eylea administered directly into the eye, typically every 4 to 12 weeks. These injections work by blocking the vascular endothelial growth factor that drives the abnormal blood vessel growth. The treatment doesn't reverse damage already done, but it can stabilize vision and prevent further loss for many patients. The American Academy of Ophthalmology's overview of dry vs wet AMD covers this in additional clinical detail.
- Prevalence
- Dry AMD: ~85–90% of cases
- Wet AMD: ~10–15% of cases
- Progression speed
- Dry AMD: Gradual (years)
- Wet AMD: Rapid (days to weeks)
- Cause
- Dry AMD: Drusen, thinning of macula
- Wet AMD: Abnormal blood vessel growth
- Standard treatment
- Dry AMD: No FDA drugs for early/intermediate; lifestyle and nutrition
- Wet AMD: Anti-VEGF injections
- Reversible?
- Dry AMD: Damage permanent; progression can be slowed
- Wet AMD: Stabilization possible with treatment
What Causes Macular Degeneration?
Macular degeneration doesn't have a single cause. It's the result of several biological processes that compound over decades. Researchers have identified at least six interacting factors that contribute to its development:
- Aging itself. The retina is the most metabolically active tissue in the human body by weight. Over a lifetime, the cellular machinery of the macula accumulates wear that the eye's repair systems can't fully reverse.
- Oxidative stress. The macula is constantly exposed to light and oxygen — a combination that generates unstable molecules called free radicals. Over time, these damage retinal cells faster than the eye's antioxidant defenses can neutralize them.
- Reduced choroidal circulation. The choroid is the dense network of small blood vessels that feeds the macula with oxygen and nutrients. Blood flow through the choroid naturally declines with age, gradually depriving photoreceptor cells of what they need to maintain themselves.
- Chronic low-grade inflammation. Inflammation that persists at a low level throughout the body — and specifically within the eye — contributes to drusen formation and accelerates retinal cell damage. Inflammatory pathways are an active area of AMD research.
- Genetics. Family history accounts for an estimated 46–71% of AMD risk. Specific gene variants — particularly in the CFH, ARMS2, and HTRA1 genes — significantly increase susceptibility. If a parent or sibling has been diagnosed with AMD, your own risk is meaningfully elevated.
- Loss of macular pigment. The macula contains protective yellow pigments — lutein and zeaxanthin — that absorb harmful blue light and help neutralize free radicals. These pigments can deplete with age, poor diet, or both, reducing the macula's natural defenses.
The reason this list matters: unlike many conditions with one cause and one fix, AMD has multiple converging causes. That's why prevention and management work best as a multi-pronged approach — diet, lifestyle, monitoring, and (where appropriate) clinical interventions, rather than a single intervention. A 2018 review in The Lancet provides a comprehensive overview of the pathogenesis for clinicians and motivated readers.
Macular Degeneration Risk Factors
Some risk factors for AMD you can't change. Others are within your control — and the distinction matters, because the modifiable factors are where everyday decisions move the needle. Doctors and researchers split them into two groups for exactly this reason.
Cannot be changed
- Age. The single biggest factor. Risk climbs sharply after age 60.
- Family history. Having a parent or sibling diagnosed with AMD doubles or triples your own risk.
- Ethnicity. Caucasians have higher rates of advanced AMD than African American or Hispanic populations, per CDC Vision Health data. The reasons are partly genetic and partly related to pigment density in the retina.
- Eye color. Light-colored irises offer less natural protection against light exposure than darker ones.
- Sex. Women have a slightly higher lifetime AMD risk than men — partly because they tend to live longer, partly because of hormonal factors that researchers continue to investigate.
Can be changed
- Smoking. The most controllable risk factor. Smokers have two to three times the AMD risk of non-smokers, and former smokers see elevated risk for years after quitting. If you smoke now, stopping is the single most impactful thing you can do for your eyes.
- Diet. Western dietary patterns — high in processed foods, low in leafy greens and colorful vegetables — are associated with higher AMD rates. Mediterranean-style diets, rich in vegetables, fruits, fatty fish, nuts, and olive oil, are associated with lower rates.
- Cardiovascular health. High blood pressure, high cholesterol, and obesity all increase AMD risk because they impair the small blood vessels that nourish the macula. Managing cardiovascular health is, indirectly, managing macular health.
- UV and sun exposure. Cumulative lifetime sunlight exposure contributes to oxidative damage in the retina. UV-protective sunglasses worn outdoors year-round meaningfully reduce risk.
- Blue light from screens. Per current AAO guidance, the role of screen blue light in AMD is debated and likely smaller than once thought.
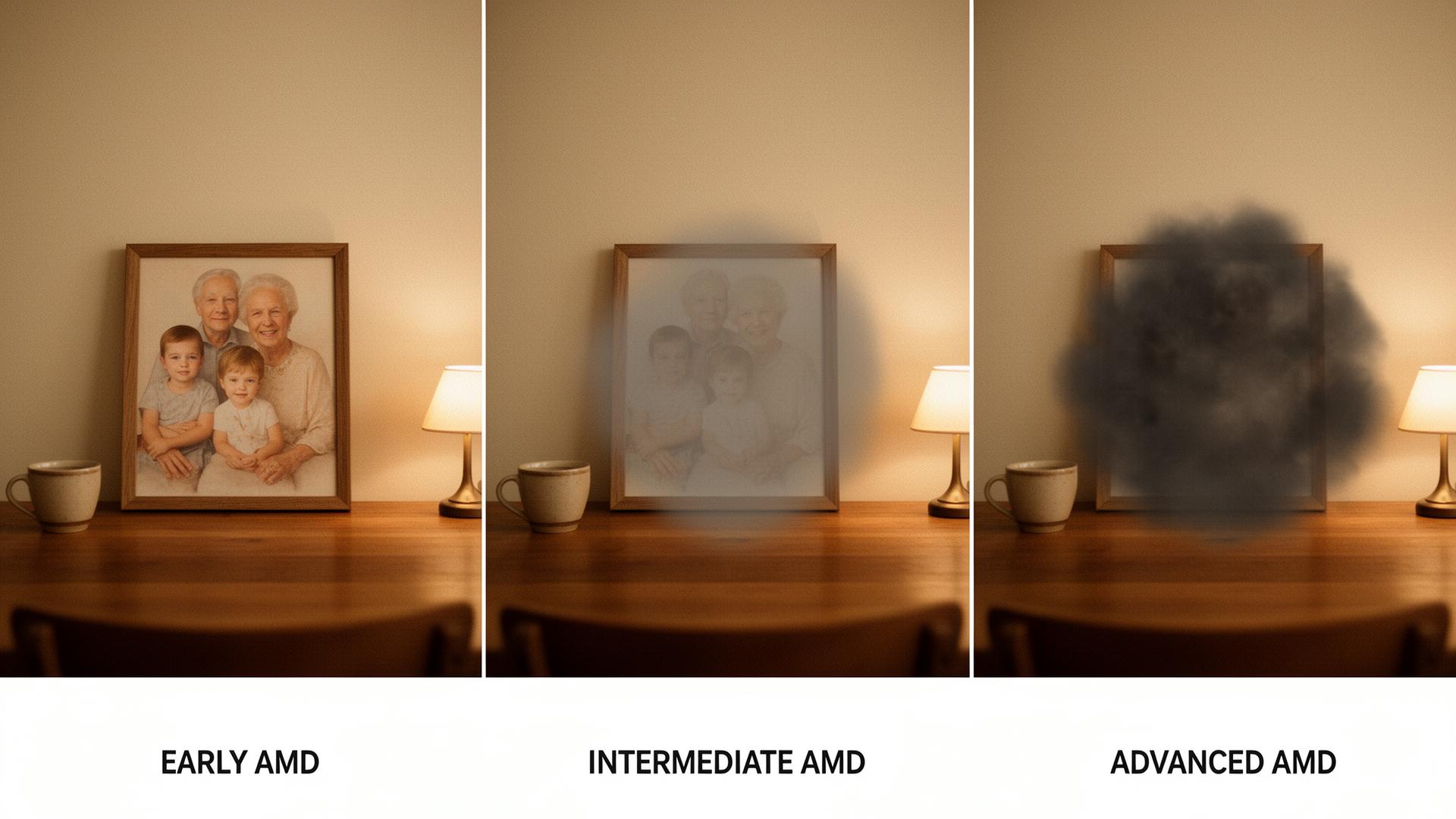
Early Symptoms of Macular Degeneration
Early AMD is often silent. By the time symptoms become obvious enough to send someone to the eye doctor, measurable damage may already have occurred. This is the practical case for regular dilated eye exams for anyone over 60 — and earlier than that for anyone with a family history. Symptoms tend to develop in three rough phases.
Early signs (often mistaken for "just getting older")
- Needing brighter light when reading or doing close work.
- More difficulty adapting from a bright environment to a dim one — for example, walking from a sunny street into a dim restaurant.
- Slightly blurred or hazy central vision.
- Colors appearing less vivid than they used to.
- Mild difficulty recognizing faces from across a room.
Intermediate signs
- A small but persistent blurry or "smudgy" spot in the center of vision.
- Words on a page appearing to have gaps or missing letters.
- Difficulty reading even with the right glasses.
- Trouble with detail tasks — sewing, threading needles, reading fine print on a prescription bottle.
Advanced signs
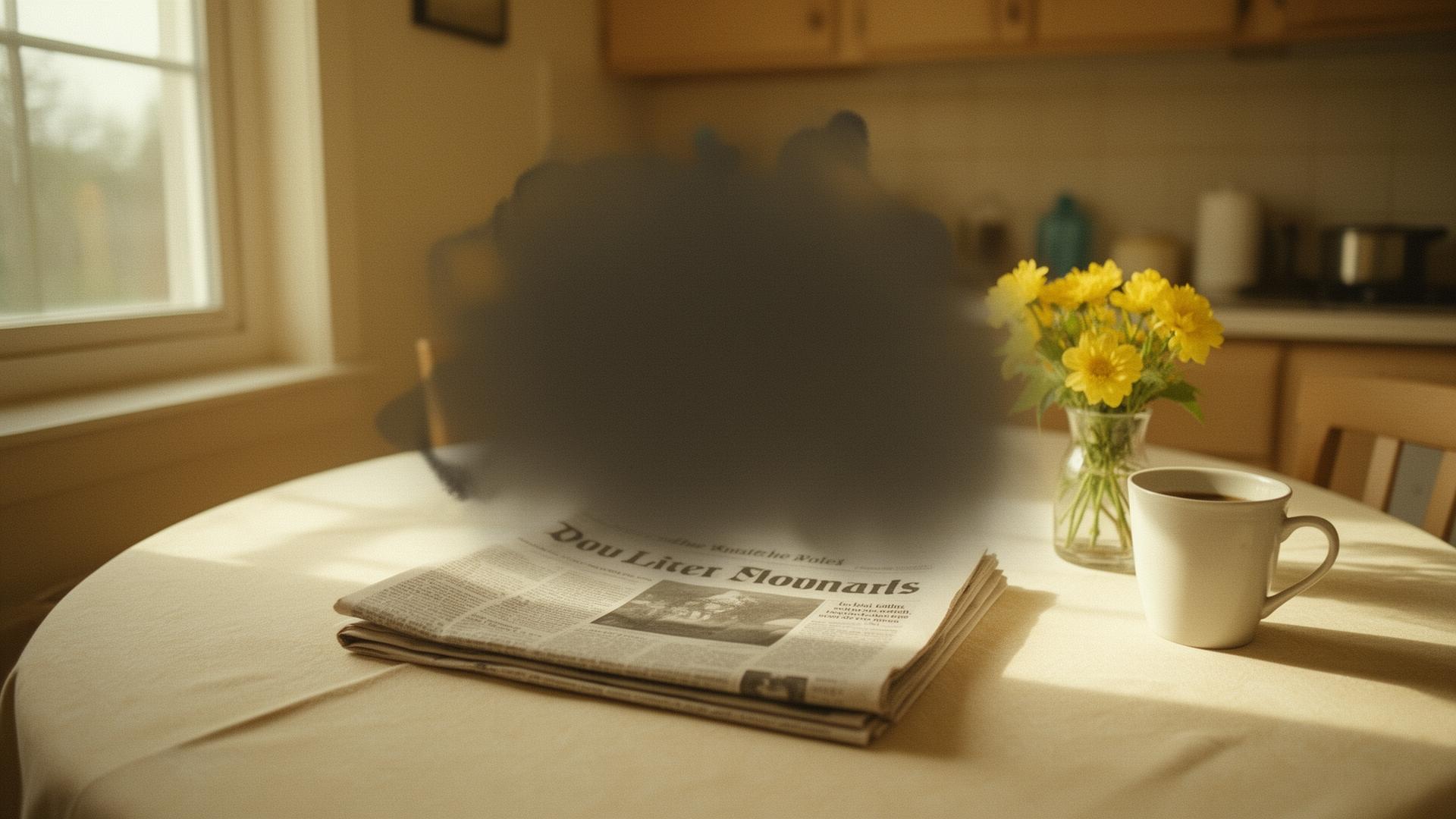
- A clearly dark, empty, or distorted spot in the center of vision.
- Straight lines — door frames, telephone poles, the edge of a book — appearing wavy, curved, or bent. This is called metamorphopsia, and it is often the first symptom of wet AMD.
- Difficulty recognizing faces even at close range.
- Significant trouble reading, driving, or watching television.
By the time symptoms become obvious, damage may already be done. Regular dilated eye exams are the only reliable way to catch early AMD.
The other important point about early symptoms is that they don't always come on symmetrically. Many people first notice changes in one eye while the other eye compensates — covering for the affected eye when both are open. The way to catch this is to close one eye at a time and look at the same scene with each eye separately. Differences between the two are the kind of finding worth mentioning at your next appointment. The AAO's patient symptoms guide covers this and other practical self-checks.
How Macular Degeneration Is Diagnosed
Diagnosing AMD is largely the work of three tools used together. None of them is uncomfortable. None of them takes long. Your eye doctor will use some combination of these — plus the standard visual acuity test you'd get at any eye appointment — to confirm whether AMD is present and at what stage.
1. Dilated eye exam
Drops are placed in each eye to widen the pupils, which gives the doctor a clear view of the retina. Once the drops have taken effect — usually 20–30 minutes — the doctor examines the back of each eye for drusen, pigment changes, signs of bleeding, or fluid. This is the foundational AMD diagnostic. Plan for some light sensitivity for two to four hours afterward, and arrange for someone else to drive you home if your appointment is in daylight.
2. Optical Coherence Tomography (OCT)
OCT is a non-invasive imaging scan that uses light waves to take detailed cross-section pictures of the retina — similar in concept to an ultrasound, but using light instead of sound. It reveals the retinal layers in fine detail, detects fluid (a hallmark of wet AMD), and allows the doctor to track progression between visits. Most retinal specialists rely on OCT to monitor AMD patients over time. The scan takes a few minutes per eye and is completely painless.
3. The Amsler grid
The simplest tool — and the one you'll use at home between appointments. The Amsler grid is a printed square of evenly spaced black lines on a white background, with a single dot in the center. You hold it at reading distance, cover one eye, and stare at the central dot. Any lines that appear wavy, broken, distorted, or missing may indicate AMD progression. Many specialists give patients a grid to use weekly. A change you notice on the grid is reason to call your doctor the same day — not wait for your next routine appointment.
Other tests your doctor may use
- Fluorescein angiography — a dye injected into the arm circulates through retinal vessels, helping identify leaking abnormal blood vessels in wet AMD.
- Fundus autofluorescence (FAF) — imaging that highlights metabolic changes and atrophic areas in the retina.
- Genetic testing — increasingly available, helpful in family-history cases or for clinical-trial enrollment, not yet routine.
A comprehensive AMD workup typically takes 60 to 90 minutes from check-in to checkout. Once a diagnosis is made, your doctor will discuss the next steps and treatment options — covered in detail in our companion guide on macular degeneration treatment.
The Stages of Macular Degeneration
Doctors stage AMD primarily by the size and number of drusen visible during the dilated exam, along with any signs of pigment change, atrophy, or wet conversion. Understanding the stages helps you understand what your diagnosis means and what's likely to come next.
Early AMD
Several small drusen, or a few medium-sized drusen, visible during a dilated exam. No pigment changes. No vision loss. Most people with early AMD have no symptoms at all and only learn they have it from a routine eye appointment. The discovery can be jarring precisely because the eyes feel completely normal — but early AMD is usually a slow-moving stage, and many people remain in it for years or decades.
Intermediate AMD
Many medium drusen, or at least one large drusen, plus possible pigment changes in the macula. Some people experience mild central vision symptoms — needing more light, slight central blur — but many remain asymptomatic. This is the stage at which standard nutritional intervention is typically discussed by ophthalmologists, based on the AREDS2 clinical trial framework. The clinical evidence and limits of that approach are covered in our deeper companion piece: The Truth About AREDS Vitamins. At this stage, the conversation also shifts toward more frequent monitoring.
Advanced AMD — two forms
Advanced AMD takes two distinct forms, with different progression patterns and different treatment options.
Geographic atrophy (advanced dry AMD). Distinct patches where retinal cells have died, leaving "atrophic" areas that no longer process visual information. Progression is gradual but irreversible. Until 2023, no FDA-approved treatments existed for geographic atrophy. Two drugs — pegcetacoplan (Syfovre) and avacincaptad pegol (Izervay) — were approved that year to slow progression. Neither reverses damage; both are administered as intravitreal injections at intervals similar to anti-VEGF therapy.
Neovascular (wet) AMD. Abnormal blood vessels grow under the retina, leaking fluid or blood into macular tissue. Untreated, wet AMD can cause rapid central vision loss within weeks. Treatment is anti-VEGF injection, as covered in Section 2. Caught early, wet AMD treatment can preserve and sometimes recover meaningful vision — which is why same-day response to the symptoms in Section 5 matters so much.
A realistic perspective is worth holding in mind. Not everyone with early or intermediate AMD progresses to advanced AMD. With monitoring, lifestyle attention, and appropriate clinical intervention, many patients remain stable for years or decades. The goal of AMD care, in most cases, is not "cure" — it's preserving the vision you have for as long as possible. That goal is achievable, and the tools for achieving it are better in 2026 than they were even five years ago.
Protecting Your Macula: What You Can Do Today
A macular degeneration diagnosis is not a verdict. It is a starting point. What you do over the months and years that follow — small daily habits, careful monitoring, the right conversations with your doctor, and the right nutritional support — meaningfully shapes how the condition progresses. The research is clearer than most patients realize on what actually helps. Here is what it says.
The lifestyle foundation
None of these are dramatic. The research is just consistent across decades of AMD studies.
- Stop smoking if you currently do. The single biggest controllable factor, as Section 4 covered. Smokers face two to three times the AMD risk of non-smokers. Quitting at any age reduces ongoing risk meaningfully.
- Adopt a Mediterranean-style diet. Leafy greens (kale, spinach, collards), colorful vegetables, fatty fish (salmon, sardines, mackerel), nuts, olive oil, whole grains. Multiple large observational studies have linked this dietary pattern to reduced AMD progression.
- Manage your cardiovascular health. Blood pressure, cholesterol, body weight. The small blood vessels that feed the macula reflect the health of every other vessel in the body.
- Wear UV-protective sunglasses year-round. Even on overcast days. Cumulative UV exposure has solid evidence behind it.
- Stay physically active. Regular moderate exercise — walking, swimming, cycling, gardening — supports vascular health throughout the body, eyes included.
The role of targeted nutritional support
Beyond lifestyle, the question of nutritional supplementation comes up at nearly every intermediate AMD diagnosis. The reason is research, not marketing. Specific nutrients have been studied for their role in macular health for over 25 years.
The landmark research is the Age-Related Eye Disease Study (AREDS) and AREDS2, conducted by the National Eye Institute over multiple decades and more than 4,000 participants. The trials demonstrated that a specific combination of antioxidants — lutein, zeaxanthin, vitamins C and E, zinc, and copper — could reduce the risk of progression to advanced AMD by approximately 25% in patients with intermediate AMD. The original AREDS formula included high-dose beta-carotene, which AREDS2 replaced with lutein and zeaxanthin after research linked beta-carotene supplementation to increased lung cancer risk in former smokers. The updated AREDS2 publication appeared in JAMA in 2013 and remains the clinical reference point.
Why formula matters
A point most patients learn the hard way: not all supplements marketed as "AMD support" are built around the AREDS2 evidence. Off-the-shelf supplements vary widely in their ingredient list, the dose of each ingredient, and the form of zinc used (some forms cause stomach upset; others are well-tolerated). Many older "eye health" products still use the original AREDS formula, beta-carotene and all. Some skip the carotenoids entirely. Reading the label carefully — and comparing it against the AREDS2 nutrient set — is worth doing.
The more interesting question — beyond simply replicating the AREDS2 formula — is whether a more comprehensive formula can address the converging causes of AMD we covered in Section 3, rather than just one or two of them.
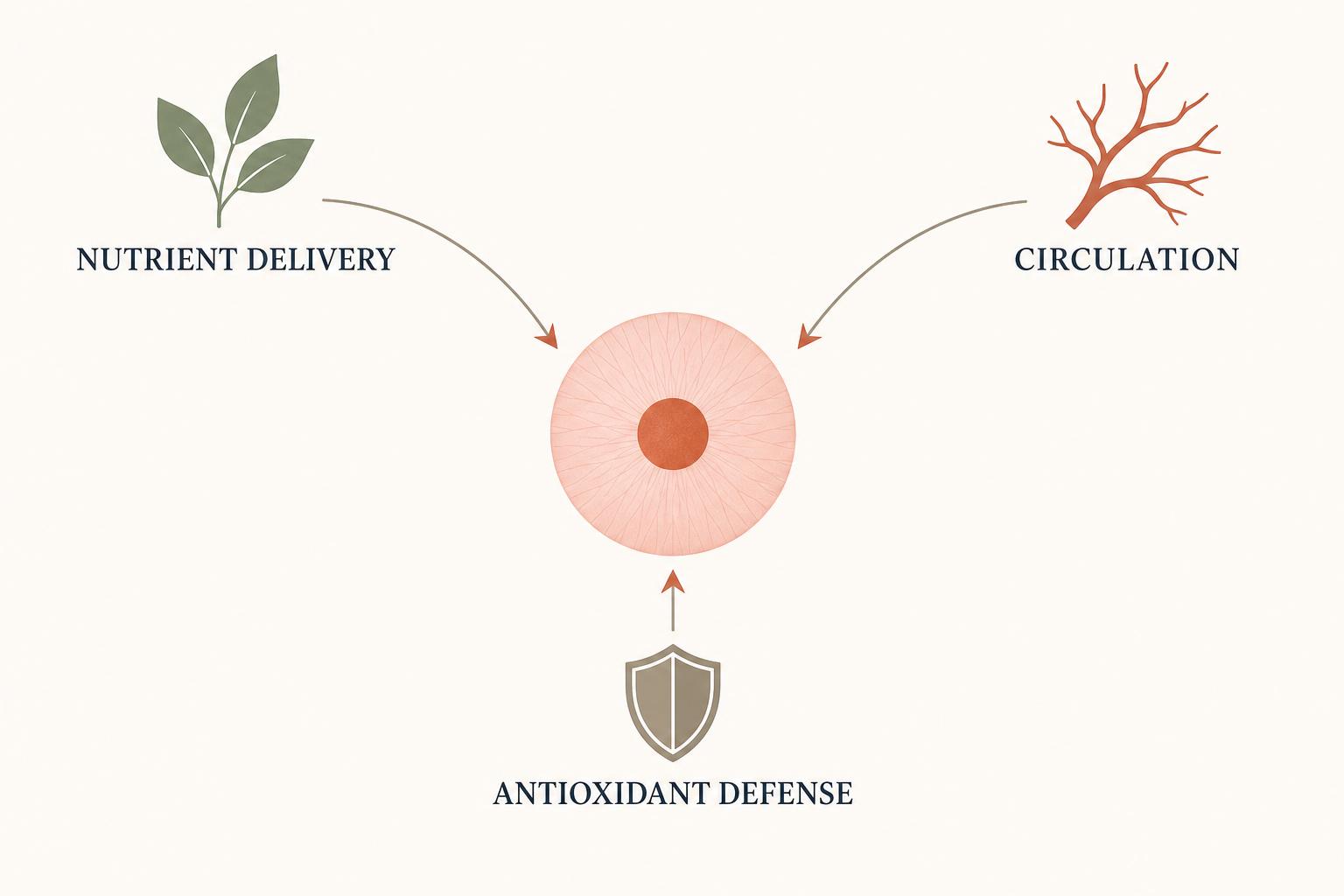
A more comprehensive approach: three pathways
Current AMD research consistently points to three broad pathways where targeted nutrients can support macular health. Think of these as the three places the macula needs help, not as a single intervention.
- Nutrient delivery to the retina. Macular pigments (lutein, zeaxanthin) and key antioxidants (vitamins C and E, zinc) absorb harmful light and protect retinal cells from oxidative damage. This is the pathway AREDS2 directly addresses.
- Circulation to the choroid. The dense network of small blood vessels feeding the macula benefits from nutrients that support vascular tone and microcirculation — a pathway AREDS2 was not designed to address but that research increasingly recognizes as central to AMD progression.
- Antioxidant defense at the cellular level. Beyond the macula's pigment shield, broader antioxidant support helps neutralize free radicals throughout retinal tissue and supports the cellular machinery that has to keep working through aging.
A formula that addresses all three pathways — rather than just one — aligns more closely with what current research describes as the actual pathophysiology of AMD progression. The challenge for patients is finding one.
One formula we recommend our readers consider as part of this conversation with their doctor is Vision Enhance Pro — a 24-ingredient daily formula developed by BioPeak Lab to address all three pathways in a single capsule. It includes the full AREDS2-validated nutrient set at clinical doses, plus additional ingredients targeting choroidal circulation and broader antioxidant defense. We've reviewed the formula's ingredient logic against the AREDS2 evidence base and the broader AMD research literature, and it's the most comprehensive consumer formula we've encountered that's grounded in the science rather than in marketing.
If you decide to explore it, bring the ingredient list to your eye doctor or primary physician before starting. Any new supplement deserves a brief medical conversation, especially if you're taking other medications.
Closing perspective
AMD is one of the most actively researched conditions in eye medicine. Treatment options are better in 2026 than they were five years ago, and they will be better still in 2030. You are not powerless. You are not alone.
Whatever you decide about supplementation, the foundation stays the same: build a monitoring relationship with a retinal specialist, use the Amsler grid weekly, manage the lifestyle factors within your reach, and treat any sudden change in central vision as a same-day reason to call your doctor. The macula is small. The work of protecting it is steady, patient, and largely unglamorous. It is also, by and large, work that pays off — in years of preserved sight, in the things you can still do, in the faces you can still recognize.
A formula designed for the three pathways of macular health
Read our complete review of Vision Enhance Pro — a 24-ingredient daily formula developed by BioPeak Lab to support nutrient delivery, choroidal circulation, and antioxidant defense in a single capsule.
Learn more about Vision Enhance Pro →Independent editorial recommendation. We do not accept payment for product reviews on eyehealth-today.com.
Related articles from eyehealth-today.com

The Truth About AREDS Vitamins: What the Research Actually Shows
A clear-eyed look at AREDS2, what it proves, what it doesn't, and where the science of macular nutrition has moved since 2013.
Read the guide →

Macular Degeneration Treatment Options Explained
From watchful waiting to anti-VEGF injections to the new geographic atrophy drugs — the current treatment landscape, in plain language.
Read the guide →
Diet for Macular Degeneration: What to Eat and Avoid
Coming soon — a practical Mediterranean-style eating guide for AMD patients.